Pudendal Neuralgia: Symptoms, Causes & At-Home Relief
Based on the Nantes criteria (Labat et al. 2008), peer-reviewed clinical research, and pelvic floor physical therapy guidelines. See our editorial standards.
Quick Answer
Pudendal neuralgia is neuropathic pain caused by irritation of the pudendal nerve, which supplies the perineum, genitals, and rectum. Its hallmark: burning or stinging pain that worsens when sitting and improves when standing. It affects men and women equally and responds to a combination of pelvic PT, nerve-calming medications, and lifestyle adjustments.
In this article
What Is the Pudendal Nerve?
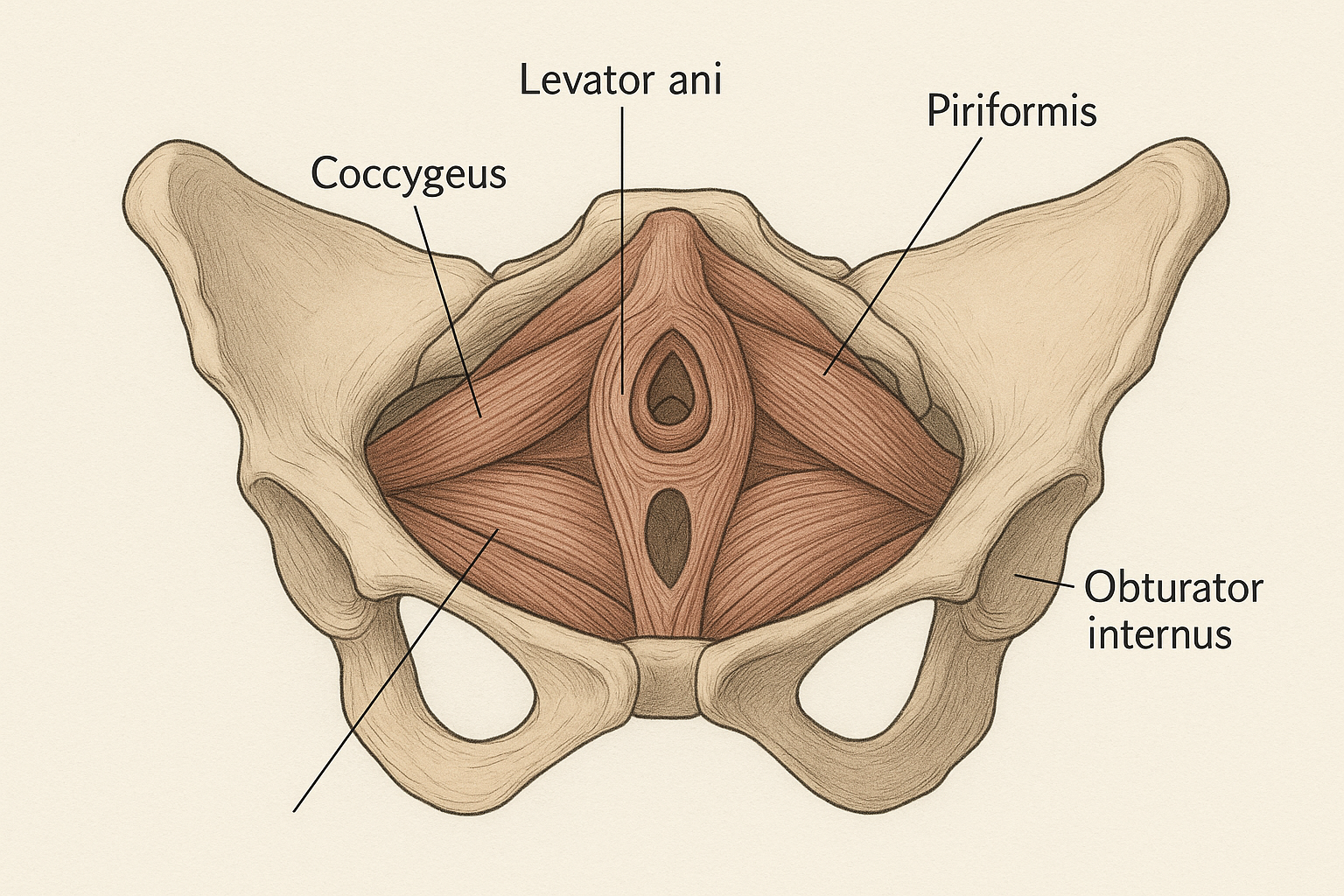
The pudendal nerve is the primary sensory and motor nerve of the perineum — the region between the genitals and the anus. It originates from the sacral nerve roots S2, S3, and S4, exits the pelvis through the greater sciatic foramen, wraps around the sacrospinous ligament, and re-enters through the lesser sciatic foramen to travel through Alcock's canal — a fibromuscular tunnel formed by the obturator internus muscle on the lateral pelvic wall.
The pudendal nerve has three main branches, each supplying a distinct region:
- The inferior rectal nerve: supplies the external anal sphincter and perianal skin
- The perineal nerve: supplies the perineal muscles, scrotum or labia majora, and urethra
- The dorsal nerve of the clitoris or penis: supplies the clitoris (in women) or the dorsum of the penis (in men), and is responsible for sexual sensation and response
Because the pudendal nerve supplies such a wide and sensitive territory — including the genitals, urethra, external sphincters, and rectum — irritation or entrapment of this nerve produces an equally wide and distressing range of symptoms that often appear unrelated to one another. Understanding the nerve's anatomy is essential to understanding why pudendal neuralgia mimics so many other conditions and why it is so frequently misdiagnosed [1].
What Is Pudendal Neuralgia?
Pudendal neuralgia is neuropathic pain arising from irritation, compression, or entrapment of the pudendal nerve anywhere along its course from the sacral roots through Alcock's canal to its terminal branches. The term "neuralgia" means nerve pain — specifically, the burning, electric, or stabbing quality of pain that is characteristic of nerve involvement, distinct from musculoskeletal ache.
The condition is sometimes called pudendal nerve entrapment (PNE) when a structural compression of the nerve — typically at Alcock's canal — is identified, though many clinicians use pudendal neuralgia as the broader diagnostic term covering both entrapment and non-entrapment irritation.
Pudendal neuralgia affects approximately 1% of the general population, though the true prevalence is likely higher due to widespread underdiagnosis [1]. It affects men and women in roughly equal numbers — a fact that surprises many patients and providers who associate pelvic pain primarily with women. The average time from symptom onset to diagnosis is reported to be 3–5 years in multiple studies, reflecting the diagnostic difficulty of this condition.
The 5 Nantes Criteria
In 2008, Labat et al. published a consensus paper defining the diagnostic criteria for pudendal neuralgia, now known as the Nantes criteria [1]. These five criteria are used by clinicians worldwide to identify pudendal neuralgia from the clinical history alone, before any investigation. All five must be present for a definitive diagnosis; cases meeting most but not all criteria are considered "possible pudendal neuralgia."
- Pain in the anatomical territory of the pudendal nerve. Pain must be located in the perineum (between the genitals and anus), the external genitalia (vulva, clitoris, penis, or scrotum), or the anus and rectum. Pain elsewhere — such as in the buttocks, hips, or lower back — does not fulfill this criterion unless it co-exists with perineal symptoms.
- Pain worsened by sitting. This is the most clinically distinctive feature of pudendal neuralgia. Sitting compresses the pudendal nerve in Alcock's canal, directly worsening neuropathic pain. The pain characteristically improves upon standing or lying down. People with pudendal neuralgia frequently stand at their desk, avoid car journeys, and find that their longest pain-free periods occur in bed.
- Pain does not wake the patient from sleep. Unlike musculoskeletal pain, which is often worst at night or on waking, pudendal neuralgia is typically relieved by lying down. Pain that reliably wakes a person from sleep suggests an alternative diagnosis. (Note: falling asleep is still possible when lying — the point is that the pain does not typically interrupt sleep.)
- No objective sensory loss on examination. Pudendal neuralgia causes pain and altered sensation (hypersensitivity, allodynia), but not the measurable loss of touch, pinprick, or temperature sensation that would indicate nerve damage (neuropathy). If objective sensory loss is found, nerve damage rather than irritation should be considered.
- Positive diagnostic pudendal nerve block. Injection of local anesthetic around the pudendal nerve (at the ischial spine) that produces temporary but significant pain relief confirms pudendal nerve involvement and supports the diagnosis. This criterion is confirmatory rather than required for clinical diagnosis in all settings.
Symptoms in Women
In women, pudendal neuralgia presents with a characteristic cluster of symptoms that can affect quality of life profoundly, disrupting work, relationships, and sexual health. Because these symptoms overlap with conditions like vulvodynia, interstitial cystitis, and endometriosis, misdiagnosis is common.
- Vulvar burning. A persistent burning, stinging, or rawness in the vulva (labia, vaginal entrance, or perineum) that is often described as feeling like a sunburn or chemical irritation, without visible inflammation to explain it.
- Clitoral pain or hypersensitivity. The dorsal nerve of the clitoris is a terminal branch of the pudendal nerve. Its irritation produces clitoral pain, persistent genital arousal without desire (in some cases), or extreme sensitivity to touch that makes clothing contact intolerable.
- Dyspareunia (painful intercourse). Pain during or after vaginal penetration, caused by both the nerve's hypersensitivity and the co-existing pelvic floor muscle tension that frequently accompanies pudendal neuralgia. Pain is often worst in the 24–48 hours after intercourse.
- Vaginal tightness or spasm. Pudendal neuralgia frequently co-exists with hypertonic pelvic floor dysfunction. The nerve's involvement in motor function can contribute to pelvic floor muscle guarding and vaginismus-like presentations.
- Urinary urgency and frequency. The pudendal nerve supplies the external urethral sphincter and contributes to bladder sensation. Its irritation can produce urge symptoms that mimic overactive bladder, often without a positive urine culture or abnormal cystoscopy.
- Painful tampon insertion. Insertion of a tampon — or any penetrative object — may trigger sharp, burning pain at the vaginal entrance, reflecting the nerve's hypersensitivity in the perineal branch territory.
- Rectal pain or burning. Involvement of the inferior rectal branch produces anorectal burning, pain with defecation, or rectal fullness and pressure that may be mistaken for hemorrhoids or rectal conditions.
- Perineal aching. A dull, constant ache in the perineal body — the muscular structure between the vagina and anus — that worsens with prolonged sitting and improves when standing.
- Increased pain after sexual activity. Orgasm, which involves rhythmic contraction of the pelvic floor muscles and pudendal nerve involvement, frequently triggers a pain flare lasting hours to days in women with pudendal neuralgia.
Symptoms in Men
In men, pudendal neuralgia is one of the most common underlying diagnoses in chronic pelvic pain syndrome — a diagnosis that is itself frequently mislabeled as chronic prostatitis. Men often go years without a correct diagnosis because awareness among urologists and GPs of pudendal nerve involvement in male pelvic pain remains limited [2].
- Penile or scrotal burning. A burning, stinging, or electric-shock quality pain in the penis (shaft or tip) or scrotum, often without visible cause. The pain may be intermittent or constant.
- Perineal ache. A dull pressure or aching sensation in the area between the scrotum and anus — the perineal body — that worsens markedly with sitting.
- Rectal pain or burning. Anorectal burning, pain with defecation, or rectal pressure, driven by irritation of the inferior rectal branch. This is sometimes mistaken for hemorrhoids, fissures, or proctitis.
- Urinary hesitancy or weak stream. Pudendal nerve involvement in the external urethral sphincter can cause difficulty initiating urination, a weak or interrupted stream, or the sensation of incomplete emptying — symptoms that commonly lead to a prostate evaluation before the pudendal nerve is considered.
- Pain after ejaculation. Ejaculation involves pudendal nerve-mediated pelvic floor contractions. In men with pudendal neuralgia, ejaculation frequently triggers a significant pain flare lasting minutes to days. This symptom, combined with perineal ache, is among the strongest clinical indicators of pudendal nerve involvement in male pelvic pain.
- Sitting pain. Pain in the perineum or under the sit bones that builds with prolonged sitting — in a car, at a desk, or on a bicycle — and improves within minutes of standing. This positional pattern is the hallmark of pudendal nerve compression.
- Urinary frequency and urgency. Needing to urinate frequently without a full bladder, and experiencing strong urge signals that are difficult to suppress. Often attributed to benign prostatic hyperplasia or overactive bladder before the pudendal nerve is assessed.
- Scrotal hypersensitivity. The scrotal skin supplied by the perineal branch of the pudendal nerve may become hypersensitive — even light touch or clothing contact on the scrotum triggers pain or burning.
Frequently Misdiagnosed
Pudendal neuralgia is frequently misdiagnosed as prostatitis (in men) or vulvodynia (in women). If you have been treated for either of these conditions without meaningful improvement, ask your provider specifically about pudendal nerve assessment — including whether a diagnostic nerve block would be appropriate for your case.
Causes and Risk Factors
Pudendal neuralgia arises from mechanical compression, chemical irritation, or ischemic injury of the pudendal nerve anywhere along its course. The following six causes account for the majority of cases.
1. Prolonged Cycling — Alcock's Canal Compression
Cycling is the most extensively studied mechanical cause. A narrow bicycle saddle places sustained pressure directly on the perineum, compressing the pudendal nerve in Alcock's canal. Studies have demonstrated nerve conduction abnormalities in cyclists with perineal symptoms [2]. Road cyclists, competitive cyclists, and people who use indoor cycling equipment for prolonged daily sessions are at highest risk. Wider saddles with a central cutout significantly reduce pudendal nerve compression.
2. Childbirth
Vaginal delivery — particularly prolonged pushing, instrumental delivery (forceps or vacuum), or large fetal head circumference — can stretch or compress the pudendal nerve as it passes through the birth canal. Pudendal nerve injury is detected in electrophysiological studies in a significant proportion of women after first vaginal delivery. Most recover fully; some develop persistent pudendal neuralgia, particularly after multiple deliveries or complicated deliveries.
3. Pelvic Surgery
Surgery in the pelvic region — including mesh implantation for prolapse or incontinence, hysterectomy, prostatectomy, or anorectal surgery — can injure or entrap the pudendal nerve through direct trauma, scar tissue formation, or suture placement near the nerve. Post-surgical pudendal neuralgia is often delayed in onset by weeks to months as scar tissue forms.
4. Habitual Prolonged Sitting
Long daily sitting — at desks, in vehicles, or during computer work — can chronically compress the pudendal nerve. This is increasingly recognized as a driver of pudendal neuralgia in office workers and remote workers, particularly in combination with a tight pelvic floor that narrows the space available to the nerve in Alcock's canal.
5. Sacral Nerve Root Compression
Disc herniation, sacroiliac joint pathology, or sacral insufficiency fractures can irritate the S2-S4 nerve roots from which the pudendal nerve originates. In these cases, pudendal neuralgia is secondary to a spinal or sacral cause, and spinal imaging is part of the diagnostic workup.
6. Pelvic Floor Hypertonicity
A chronically over-contracted pelvic floor — particularly the obturator internus and piriformis muscles that border Alcock's canal — can mechanically compress the pudendal nerve through sustained muscle tension. This is one of the reasons that hypertonic pelvic floor dysfunction and pudendal neuralgia so frequently co-exist, and why pelvic floor downtraining is a core component of pudendal neuralgia treatment.
How Is It Diagnosed?
Pudendal neuralgia is a clinical diagnosis — meaning it is made primarily from the patient's history and symptom pattern, rather than from a blood test, scan, or single objective measure. The Nantes criteria (above) provide the diagnostic framework most widely used by pelvic pain specialists.
A standard diagnostic evaluation includes:
- Detailed symptom history: The clinician will ask specifically about the location, quality, and timing of pain — particularly its relationship to sitting, standing, and lying — as well as any triggering events (surgery, childbirth, cycling) and any treatments already tried.
- Pelvic floor assessment: A pelvic floor physiotherapist or physician will assess pelvic floor muscle tone internally, look for trigger points in the obturator internus and piriformis, and map any areas of nerve hypersensitivity along the pudendal nerve territory.
- Pudendal nerve block: Injection of local anesthetic near the ischial spine (a bony landmark the pudendal nerve wraps around) is both diagnostic and therapeutic. If the block produces significant temporary pain relief, this confirms pudendal nerve involvement.
- Imaging: MRI neurography (high-resolution nerve imaging) can sometimes visualize nerve abnormalities, though normal imaging does not rule out pudendal neuralgia. Sacral and lumbar spine imaging may be ordered to exclude a spinal cause.
Because this condition is poorly recognized in primary care, a referral to a pelvic pain specialist, urogynecologist, colorectal surgeon with a pelvic pain interest, or specialized pelvic floor physiotherapist is often necessary to obtain an accurate diagnosis.
Conservative Treatment Options
Most clinical guidelines recommend a conservative, multimodal approach as the first-line treatment for pudendal neuralgia, beginning with the least invasive interventions. Surgery is rarely the first option and is reserved for confirmed nerve entrapment that fails to respond to conservative measures.
Pelvic Floor Physical Therapy
A pelvic floor PT is the most important provider in the conservative management of pudendal neuralgia. Treatment includes manual release of trigger points in the obturator internus and piriformis (the muscles that border Alcock's canal), internal pelvic floor downtraining to reduce compression of the nerve, connective tissue mobilization, and neural desensitization techniques. A systematic review by Stav et al. (2012) found that pelvic floor PT produced significant symptom improvement in the majority of patients with pudendal neuralgia when followed consistently [2].
Nerve-Modulating Medications
Neuropathic pain does not respond well to standard pain relievers (NSAIDs, paracetamol). Medications that calm nerve signaling are more effective. Commonly prescribed agents include tricyclic antidepressants (amitriptyline, nortriptyline), anticonvulsants (gabapentin, pregabalin), and SNRIs (duloxetine). These are prescribed by a physician and require careful dosing titration — medication decisions are made collaboratively with your provider based on your symptom profile, other medications, and medical history.
Pudendal Nerve Block
Injection of corticosteroid and local anesthetic near the pudendal nerve at the ischial spine — performed under ultrasound or fluoroscopic guidance — can provide meaningful pain relief lasting weeks to months in many patients. Nerve blocks are typically offered in a series of 2–3 injections, spaced 4–6 weeks apart, and are often used alongside pelvic PT to create a window of reduced pain during which rehabilitation can progress more effectively.
Psychological Support
Chronic neuropathic pain involves central sensitization — the nervous system's pain processing amplifies over time. Cognitive behavioral therapy (CBT) for pain, acceptance and commitment therapy (ACT), and pain education are evidence-based components of pudendal neuralgia treatment. They do not imply that the pain is "psychological" — they address the brain's role in pain modulation, which is altered in all chronic pain conditions regardless of their physical cause.
6 At-Home Relief Techniques
These techniques complement professional treatment and can be practiced daily to manage symptoms and support nerve healing. They focus on reducing mechanical compression of the nerve, downtraining the pelvic floor muscles that border Alcock's canal, and calming the nervous system's hypersensitized response.
Technique 1: Diaphragmatic Breathing
Why it helps: Slow diaphragmatic breathing activates the parasympathetic nervous system, reduces pelvic floor muscle tone, and directly decreases the mechanical pressure on the pudendal nerve from hypertonic pelvic floor muscles. It is the most accessible and lowest-risk intervention available.
- Lie on your back with knees bent and feet flat.
- Place one hand on your belly, one on your chest.
- Inhale slowly through the nose for 4 counts — the belly hand rises, the chest hand stays still.
- As you inhale, consciously feel the pelvic floor soften and drop downward.
- Exhale through pursed lips for 6 counts, allowing a natural return to resting.
- Complete 10 breath cycles, 4 times daily. This is your foundation technique — practice it before any other technique.
Technique 2: Sitting Modifications
Why it helps: Reducing mechanical compression of the pudendal nerve during unavoidable sitting is a critical management strategy. The nerve is compressed in Alcock's canal when the sit bones bear weight on a flat surface.
- Use a cut-out cushion: A coccyx (donut) or U-shaped foam cushion removes pressure from the perineum while supporting the sit bones. This is the most effective sitting modification for pudendal neuralgia.
- Sit to one side: Shifting your weight to one side temporarily decompresses the nerve on the other. Alternate sides frequently.
- Limit sitting duration: Aim to stand or walk for 5–10 minutes every 30–40 minutes of sitting. Set a timer if needed.
- Inclined forward sitting: Tilting the seat slightly forward (3–5 degrees) redistributes weight from the perineum to the thighs. A wedge cushion can achieve this.
Technique 3: Pelvic Floor Downtraining — Reverse Kegel in Side-Lying
Why it helps: Reducing pelvic floor hypertonicity decreases muscle compression of the pudendal nerve in Alcock's canal. The side-lying position is particularly useful for people in significant pain because it completely decompresses the perineum. For a full guide to this technique, see our article on reverse kegel exercises.
- Lie on your side with a pillow between your knees for support.
- Take a slow inhale through the nose.
- As you inhale, consciously release and lengthen your pelvic floor — imagine opening outward, like a flower. The sensation is a gentle downward-and-outward expansion.
- Hold the lengthened position for 5 seconds at the top of the inhale.
- Exhale slowly and return to neutral without contracting.
- Complete 10 repetitions twice daily.
Technique 4: Hip Flexor and Piriformis Stretch
Why it helps: The piriformis muscle sits directly adjacent to the pudendal nerve's path. When tight, it can compress the nerve or its branches. Releasing the piriformis and hip flexors reduces neural compression and improves the space available to the pudendal nerve.
Piriformis stretch (supine figure-four):
- Lie on your back with both knees bent.
- Cross your right ankle over your left knee, creating a figure-four shape.
- Flex the right foot and gently press the right knee away from your body.
- For a deeper stretch, clasp your hands behind your left thigh and gently draw both legs toward your chest until you feel a stretch in your right outer hip and buttock.
- Hold for 30–45 seconds, breathing slowly. Repeat on the other side. Perform 2–3 sets per side, once daily.
Technique 5: Cold or Warm Therapy
Why it helps: Thermal application can modulate neuropathic pain signals. Cold reduces nerve conduction velocity (temporarily numbing hypersensitive signals); warmth increases local blood flow and reduces muscle spasm. Individual response varies — some people with pudendal neuralgia respond better to cold, others to warmth. Experiment carefully.
- Cold application: Wrap an ice pack or bag of frozen peas in a thin cloth. Apply to the perineum for 10 minutes maximum. Never apply ice directly to skin. Use in the first 24 hours after an activity flare.
- Warmth: A warm compress, hot water bottle in a cloth cover, or warm bath can relax pelvic floor muscles and reduce spasm-driven neural compression. Apply for 15–20 minutes.
- Alternate cold and warm (contrast therapy) may provide enhanced relief for some people — 10 minutes each, repeated 2–3 times.
Technique 6: Activity Pacing — Flare Management Protocol
Why it helps: Pudendal neuralgia responds poorly to boom-bust activity patterns — doing too much on good days and collapsing on bad days. Pacing — doing a consistent, manageable amount regardless of pain level — prevents sensitization flares and gradually expands your activity tolerance.
- Identify your baseline: Find the level of sitting and activity you can consistently tolerate without triggering a significant flare. This is your starting baseline.
- Increase by 10% per week: Gradually increase sitting tolerance, walking duration, or activity level by approximately 10% per week — regardless of whether you feel you could do more.
- Flare management: During a flare, reduce activity to 50–70% of your baseline (not to zero) and return to baseline within 3–5 days. Complete rest prolongs sensitization.
- Track triggers: Keep a simple daily log of activities and pain levels to identify patterns. Common triggers include prolonged sitting, cycling, sexual activity, stress, and certain foods (for those with co-existing IC).
Recovery Timeline
Recovery from pudendal neuralgia is rarely linear. Setting realistic expectations — and understanding that neuropathic pain takes longer to resolve than musculoskeletal pain — helps reduce frustration and supports consistent treatment adherence.
| Phase | Timeframe | Goals | Key Interventions |
|---|---|---|---|
| Pain education | Weeks 1–4 | Understand the condition; reduce fear-avoidance; establish daily breathing practice | Diaphragmatic breathing, sitting modifications, pain education resources |
| Active rehabilitation | Weeks 5–12 | Reduce pelvic floor hypertonicity; improve activity tolerance; begin nerve desensitization | Pelvic floor PT (manual + downtraining), reverse kegels, piriformis stretch, nerve block if indicated |
| Plateau assessment | Months 3–6 | Consolidate gains; assess need for medication adjustment or additional injections | Continue PT, medication review, psychological support if needed, activity pacing |
| Advanced interventions | 6+ months (if needed) | Address cases with insufficient response to conservative care | Repeat nerve blocks, neuromodulation (sacral nerve stimulation), surgical decompression for confirmed PNE |
Timeline adapted from Stav et al. 2012 and clinical practice guidelines from the International Pelvic Pain Society.
Frequently Asked Questions
What are the first signs of pudendal neuralgia?
The earliest signs are typically a burning, stinging, or electric-shock quality sensation in the perineum — the area between the genitals and the anus — or in the clitoris, vulva, penis, or rectum. The pain characteristically worsens with prolonged sitting and improves when standing or when sitting on a toilet seat, which decompresses the pudendal nerve by supporting the sit bones but leaving the perineum unsupported. Numbness or hypersensitivity (where light touch feels painful) in the same region may also appear early. If you recognize this pattern, ask your provider specifically about pudendal nerve assessment rather than accepting a generic diagnosis of pelvic pain.
Can stress make pudendal neuralgia worse?
Yes — psychological stress reliably worsens pudendal neuralgia for several reasons. First, stress activates the sympathetic nervous system and causes reflexive pelvic floor muscle contraction, which increases mechanical pressure on the pudendal nerve in Alcock's canal. Second, stress sensitizes the central nervous system's pain processing pathways, meaning the brain amplifies pain signals that arrive from the periphery. Third, stress disrupts sleep, reduces physical activity, and often triggers unhelpful coping behaviors — all of which worsen chronic pain. Many patients report their worst flares during high-stress periods at work or in personal life. Stress management — including diaphragmatic breathing, mindfulness, and CBT — is a recognized, evidence-based component of pudendal neuralgia management, not a luxury add-on.
How long does pudendal neuralgia last?
Duration varies widely and depends on the cause, how quickly treatment is started, and whether co-existing conditions are addressed. Cases caused by a single, identifiable compressive event — such as a cycling injury or complicated delivery — often respond well to conservative treatment within 3–6 months when the compressive source is removed and pelvic PT is begun promptly. Chronic cases lasting 2 or more years are more common in people who go undiagnosed or untreated for extended periods, because prolonged nerve irritation leads to central sensitization that is harder to reverse. With a multidisciplinary approach combining pelvic floor PT, nerve-modulating medication, and appropriate injections, most patients achieve meaningful pain reduction. Complete resolution is possible for many, particularly those with biomechanical causes, but is not guaranteed for all presentations.
Is pudendal neuralgia the same as vulvodynia?
Not exactly, though they frequently overlap. Vulvodynia is a descriptive diagnosis — chronic vulvar pain without a clearly identified cause. Pudendal neuralgia is a mechanistic diagnosis — pain arising from a specific nerve. Because the pudendal nerve supplies the vulva, pudendal neuralgia is one of the possible underlying causes of vulvodynia. An estimated 20–30% of women diagnosed with vulvodynia may have an identifiable pudendal nerve component driving their symptoms. Distinguishing between the two requires clinical assessment, including a provoked vestibulodynia mapping exam, pelvic floor muscle assessment, and potentially a diagnostic nerve block. If you have been told you have vulvodynia but have not had a nerve assessment, it is worth asking whether pudendal involvement has been specifically evaluated. See our pelvic floor FAQ for more on the distinction between overlapping pelvic pain diagnoses.
References
- Labat JJ, Riant T, Robert R, Amarenco G, Lefaucheur JP, Rigaud J. Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria). Neurourol Urodyn. 2008;27(4):306-310. doi:10.1002/nau.20505
- Stav K, Dwyer PL, Roberts L. Pudendal neuralgia. Fact or fiction? Obstet Gynecol Surv. 2009;64(3):190-199. doi:10.1097/OGX.0b013e318193a46e
- Cleveland Clinic. Pudendal Neuralgia: Symptoms, Causes, Diagnosis & Treatment. Cleveland Clinic Health Library. Reviewed 2023. Available at: https://my.clevelandclinic.org/health/diseases/22459-pudendal-neuralgia
Key Takeaways
- •Pudendal neuralgia is neuropathic pain in the territory of the pudendal nerve: perineum, genitals, and rectum — with burning pain that worsens when sitting and improves when standing.
- •The 5 Nantes criteria are the internationally recognized diagnostic framework — if your pain meets these criteria, specifically ask your provider about pudendal nerve assessment.
- •It affects men and women equally and is frequently misdiagnosed as prostatitis (in men) or vulvodynia (in women) — average time to diagnosis is 3–5 years.
- •Conservative first-line treatment — pelvic floor PT, sitting modifications, diaphragmatic breathing, and nerve-modulating medications — produces meaningful improvement in most cases.
- •Pelvic floor hypertonicity is a key driver of pudendal nerve compression — downtraining the pelvic floor is a central element of treatment, not just symptom management.
Support your pelvic floor relaxation at home
The PelvicFit pelvic floor relaxation program can help calm an overactive pelvic floor — a key driver of pudendal nerve irritation. Free, no signup required.
Start your relaxation session →About the Authors
PelvicFit Editorial Team
The PelvicFit editorial team produces evidence-based content on pelvic floor health, chronic pelvic pain, and related conditions, drawing on peer-reviewed research and clinical guidelines from leading pelvic health organizations.
Sarah Mitchell, DPT — Pelvic Floor Physical Therapist (Reviewer)
Sarah holds a Doctor of Physical Therapy degree and has 12 years of clinical experience treating pelvic floor disorders, including chronic pelvic pain, pudendal neuralgia, and hypertonic pelvic floor dysfunction. She has treated over 800 patients across a range of pelvic floor conditions.