Hypertonic Pelvic Floor: 12 Symptoms, Causes & 7 Relaxation Exercises
Based on peer-reviewed clinical research, pelvic floor physical therapy guidelines, and systematic reviews. See our editorial standards.
Quick Answer
A hypertonic pelvic floor is one where the muscles are chronically over-contracted — the opposite of weak. Instead of leaking, you may feel pelvic pain, painful sex, and urinary urgency. The fix is relaxation, not more kegels. Seven evidence-based exercises below will help.
In this article
- 1. What Is a Hypertonic Pelvic Floor?
- 2. 12 Symptoms of a Hypertonic Pelvic Floor
- 3. What Causes a Hypertonic Pelvic Floor?
- 4. How to Self-Test at Home
- 5. 7 Relaxation Exercises
- 6. 4-Week Relaxation Protocol
- 7. When Do Kegels Make It Worse?
- 8. When to See a Pelvic Floor Physical Therapist
- 9. Frequently Asked Questions
What Is a Hypertonic Pelvic Floor?
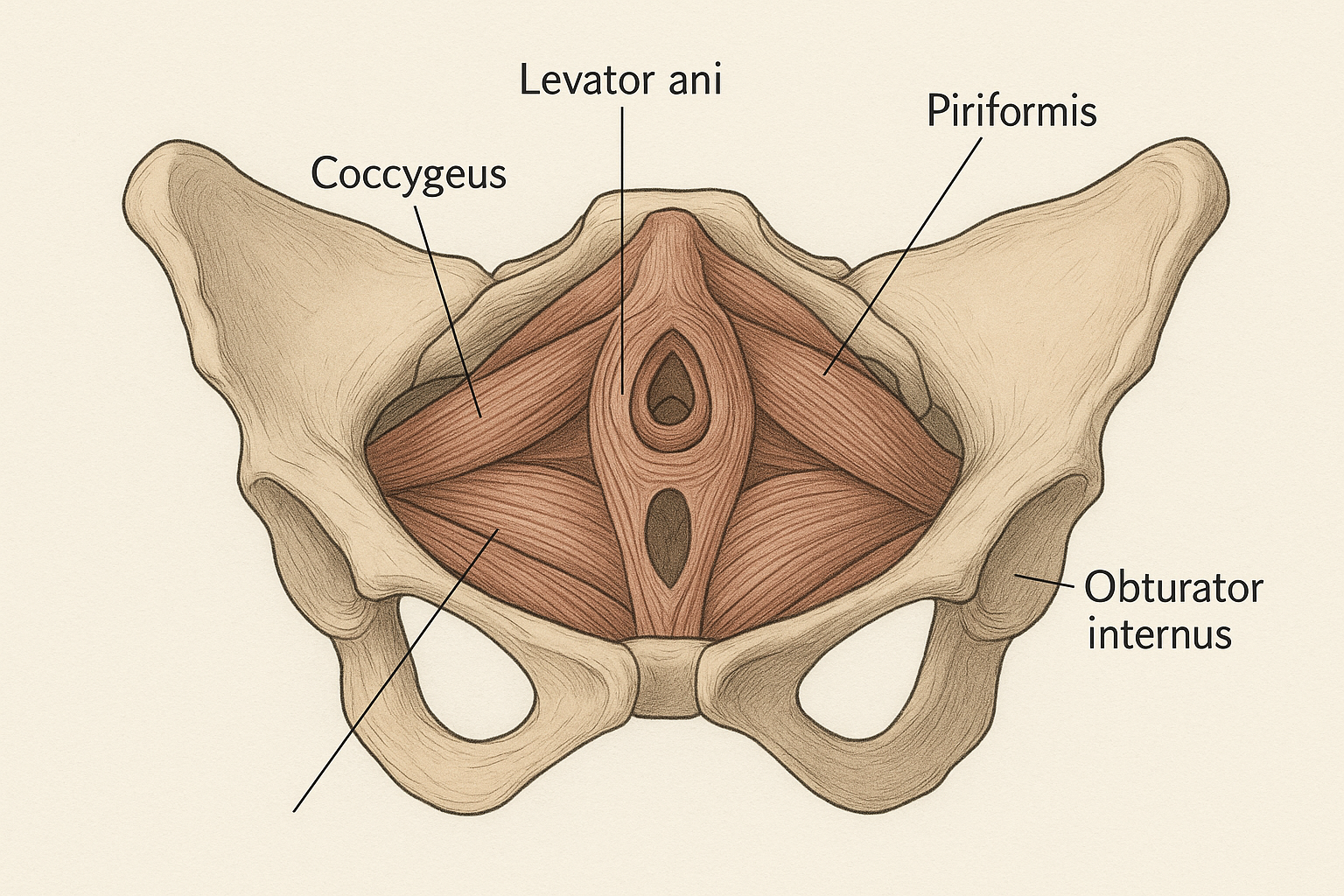
The pelvic floor is a group of muscles and connective tissues that form a hammock-like structure at the base of the pelvis, running from the pubic bone at the front to the coccyx (tailbone) at the back. These muscles support your bladder, bowel, and uterus (in women), regulate urination and defecation, and play an important role in sexual function. To understand the full anatomy, see our guide on pelvic floor muscles.
A hypertonic pelvic floor — also called an overactive, tight, or high-tone pelvic floor — is one in which these muscles are in a state of chronic, excessive contraction. The muscles cannot fully relax, even at rest. Think of it like a clenched fist that never fully opens: the tissue stays shortened, tense, and often tender.
This is the opposite of a weak (hypotonic) pelvic floor. While a hypotonic floor leads to leakage and prolapse because the muscles are too loose to provide support, a hypertonic floor causes pain and dysfunction because the muscles are too tight to function normally. The distinction matters enormously for treatment — strengthening exercises that help a weak floor will make a hypertonic floor significantly worse [1].
Hypertonic pelvic floor dysfunction is more common than many people realize. Research suggests it affects a meaningful subset of individuals presenting with chronic pelvic pain, with prevalence estimates ranging from 14–23% among people seen in pelvic floor specialty clinics [2]. Both men and women are affected, though it is diagnosed more frequently in women.
12 Symptoms of a Hypertonic Pelvic Floor
Because the pelvic floor muscles are involved in so many functions, an overactive floor produces a wide and sometimes confusing range of symptoms. The following 12 signs are the most clinically recognized presentations. You do not need to have all of them to have a hypertonic floor — even three or four of these symptoms together warrants evaluation.
- Pelvic pain or pressure. A persistent ache, heaviness, or burning sensation in the lower pelvis, perineum, or between the sit bones. This pain may be constant or triggered by activity. It is often described as a feeling of "sitting on a golf ball."
- Painful intercourse (dyspareunia). Pain during or after penetrative sex is one of the most common presentations of pelvic floor hypertonicity. The tight muscles create resistance and tenderness at the vaginal entrance or deeper in the pelvis. In men, pain during or after ejaculation is an equivalent signal.
- Vaginismus. An involuntary spasm of the pelvic floor muscles that makes penetration — by a penis, tampon, finger, or speculum — painful or impossible. Vaginismus is a manifestation of hypertonic pelvic floor muscles in women and is often successfully treated with relaxation-based pelvic floor therapy.
- Urinary urgency. A sudden, compelling urge to urinate that is difficult to defer, even when the bladder is not full. Overactive pelvic floor muscles can irritate the bladder directly and disrupt normal detrusor (bladder muscle) signaling, producing urgency without true bladder overactivity.
- Urinary frequency. Needing to urinate more than 8 times per day, or waking more than once per night to void (nocturia), when fluid intake does not explain the pattern. Pelvic floor tension keeps the pelvic region in a heightened state of activation, which can drive frequent urge signals.
- Incomplete bladder emptying. The sensation that the bladder has not fully emptied after urination, or a weak, interrupted stream. Hypertonic external urethral sphincter muscles can obstruct normal voiding, leading to hesitancy and post-void residual urine.
- Difficulty defecating or constipation. Straining to have a bowel movement, incomplete evacuation, or the need to apply perineal pressure to defecate. A hypertonic puborectalis and external anal sphincter can create a paradoxical obstruction during attempted defecation — the muscle tightens when it should relax.
- Tailbone (coccyx) pain. Pain at or around the coccyx, which may worsen with prolonged sitting. The coccygeus muscle, part of the pelvic floor, attaches directly to the coccyx, and its chronic tension pulls on the tailbone.
- Sitting discomfort. Pain, pressure, or numbness in the perineum or sit bones during seated activities, especially prolonged sitting. Many people with hypertonic floors find sitting on hard surfaces intolerable.
- Lower back pain. The pelvic floor forms the base of the core canister, working in concert with the diaphragm, transversus abdominis, and multifidus. When the pelvic floor is chronically tense, it disrupts normal lumbar and sacral movement patterns, contributing to persistent lower back pain [1].
- Pelvic muscle spasms. Involuntary, painful contractions in the pelvic floor that may come on suddenly, sometimes triggered by movement, sex, or bowel activity. These spasms can be severe and debilitating.
- Worsening symptoms with standard kegel exercises. This is perhaps the most diagnostically useful sign. If practicing kegel contractions makes your pelvic pain, urgency, or other symptoms worse rather than better, this is a strong clinical indicator that your floor is already over-contracted and does not need additional strengthening.
Important Warning
Do NOT do standard kegel exercises if you recognize these symptoms — they add more contraction to muscles that are already too tight and can make a hypertonic floor significantly worse. Switch to the relaxation exercises below and seek assessment from a pelvic floor physical therapist.
What Causes a Hypertonic Pelvic Floor?
A hypertonic pelvic floor rarely has a single cause. Most cases involve a combination of physical, psychological, and lifestyle factors that accumulate over time. Understanding the cause matters because it guides treatment: stress-driven hypertonicity, for example, responds well to breathing and mindfulness work, while post-surgical tension may require hands-on manual therapy.
1. Chronic Psychological Stress and Anxiety
The pelvic floor holds tension in response to emotional stress in the same way the jaw (TMJ) or shoulders do. When the nervous system is in a prolonged state of threat activation, the pelvic floor muscles contract reflexively and continuously. Many people with anxiety, PTSD, or chronic life stress present with significant pelvic floor hypertonicity, often without realizing they are holding tension there. Research by Faubion et al. has documented the strong association between psychological stress and pelvic floor dysfunction [2].
2. History of Pelvic Trauma or Sexual Trauma
Physical or sexual trauma — including childhood abuse, assault, or traumatic medical procedures — frequently results in chronic pelvic floor guarding. The body protects the vulnerable pelvic region through sustained muscle contraction, a pattern that can persist long after the trauma has passed. Trauma-informed care is essential when treating hypertonicity that has a trauma component.
3. High-Impact Sports with Repetitive Pelvic Loading
Running, gymnastics, CrossFit, heavy weightlifting, and cycling can all drive pelvic floor overactivity. High-impact sports demand repeated rapid contractions of the pelvic floor to protect against intra-abdominal pressure spikes, and some athletes develop chronic tension as the muscles fail to fully relax between training sessions. Elite athletes are at particular risk.
4. Endometriosis, Interstitial Cystitis, and Chronic Pelvic Pain Conditions
Pain is one of the strongest drivers of muscle guarding. When the pelvis is chronically painful from endometriosis, interstitial cystitis, irritable bowel syndrome, or other pelvic conditions, the pelvic floor muscles contract protectively around the pain source. This creates a pain-tension cycle: the underlying condition causes pain, pain drives muscle guarding, and muscle guarding generates its own pain signals, amplifying the original condition.
5. Habitual Posture and Prolonged Sitting
An anterior pelvic tilt (arched lower back), posterior pelvic tuck (tucked tailbone), or prolonged desk sitting can all create sustained pelvic floor tension. When the pelvis is in a non-neutral position for hours at a time, the pelvic floor cannot rest in its natural resting length. Over months and years, this postural pattern trains the muscles into a shortened state.
How to Self-Test at Home
A formal diagnosis of pelvic floor hypertonicity requires internal assessment by a trained pelvic floor physiotherapist. However, these three body-awareness tests can give you useful preliminary information about whether your pelvic floor may be over-contracted.
Test 1: The Breath Observation Test
Lie on your back with your knees bent and feet flat on the floor. Place one hand on your lower belly. Take a slow, deep breath in through your nose and observe what happens: the belly should expand outward as the diaphragm descends. If you notice that breathing is shallow, chest-dominant, or that your belly barely moves, this indicates tension in the diaphragm-pelvic floor system. A hypertonic pelvic floor often co-exists with restricted diaphragmatic breathing — the two structures work as a pressure system and are intimately connected.
Test 2: The Sitting Awareness Test
Sit on a hard, flat surface (not a cushioned chair). Notice whether you feel pressure, discomfort, or pain in the perineum or sit bones within 10–15 minutes of sitting. Then try sitting on a toilet seat — which supports the sit bones but leaves the perineum unsupported. If your discomfort significantly decreases on the toilet seat, this is a strong signal of pelvic floor tension (the same test used clinically for pudendal neuralgia assessment).
Test 3: The Squat Relaxation Test
Stand with feet shoulder-width apart and slowly lower into a deep squat (hold onto a doorframe for support if needed). A healthy pelvic floor should be able to relax and lengthen in this position. If you feel increased pelvic pain, tightness, or pressure in the deep squat — rather than a sense of release — this may indicate difficulty with pelvic floor relaxation. Conversely, if the squat provides relief, this is a useful position to use during your relaxation practice.
7 Relaxation Exercises for a Hypertonic Pelvic Floor
These seven exercises are the foundation of conservative treatment for pelvic floor hypertonicity. They are listed in order of priority: start with the breathing exercises before progressing to the yoga-based movements. Each exercise targets either the neuromuscular relaxation pathway or the structural lengthening of the pelvic floor muscles and their surrounding tissues.
Exercise 1: Diaphragmatic (360-Degree) Breathing
Why it works: The diaphragm and pelvic floor move as a coordinated unit. On every inhale, the diaphragm descends and the pelvic floor should eccentrically lengthen (drop). On every exhale, both structures return to their resting position. When the pelvic floor is hypertonic, this natural descent is restricted. Diaphragmatic breathing is the single most important tool for retraining pelvic floor relaxation [3].
- Lie on your back with knees bent, or sit comfortably in a chair.
- Place one hand on your chest and one on your lower belly.
- Inhale slowly through your nose for 4 counts. Focus on sending the breath to your belly — the lower hand should rise, the upper hand should stay still.
- As you inhale, consciously imagine your pelvic floor softening and dropping downward, like a hammock gently lowering.
- Exhale slowly through pursed lips for 6 counts, allowing the belly to fall naturally.
- Repeat for 10 breath cycles. Practice 3–4 times daily.
What to feel: A gradual sense of warmth and heaviness in the perineum. Over days to weeks, the pelvic floor should become more responsive to the inhale signal, dropping more readily each time.
Exercise 2: Reverse Kegel — Conscious Pelvic Floor Lengthening
Why it works: A reverse kegel is the deliberate opposite of a contraction — it is a conscious, active lengthening of the pelvic floor on the inhale. Where a standard kegel says "lift and squeeze," a reverse kegel says "open and release." This is the primary therapeutic exercise for hypertonic floors. For a complete guide, see our article on reverse kegel exercises.
- Lie on your back with knees bent, feet flat.
- Take a slow inhale through the nose for 4 counts.
- As you inhale, imagine you are gently bearing down — the sensation is similar to the beginning of urination or a bowel movement, but without straining or pushing. The pelvic floor should feel like it is expanding outward in all directions.
- Hold the lengthened position for 3–5 seconds at the end of your inhale.
- Exhale slowly and allow the muscles to return to neutral (do not actively contract on the exhale).
- Complete 10 repetitions. Practice twice daily.
Common mistake: Bearing down with force (straining). The reverse kegel should be subtle — a gentle, controlled opening, not a push.
Exercise 3: Child's Pose with Pelvic Release
Why it works: Child's pose places the pelvis in a position that naturally encourages pelvic floor lengthening. The hip flexion and internal rotation open the posterior pelvic floor (the muscles closest to the tailbone), and the supported position allows the nervous system to downregulate. Using diaphragmatic breathing in this pose amplifies the pelvic floor release.
- Kneel on a yoga mat or soft surface. Bring your big toes together and knees wide apart (wider than hip-width).
- Slowly lower your torso forward until your forehead rests on the mat. Arms can extend forward or rest alongside your body.
- Take 5 slow diaphragmatic breaths. On each inhale, focus on feeling the pelvic floor drop toward the mat.
- Hold for 60–90 seconds, breathing continuously.
- Repeat 2–3 times per session.
Modification: Place a folded blanket under your bottom if your hips do not reach your heels comfortably, or use a bolster under your torso.
Exercise 4: Happy Baby Pose
Why it works: Happy baby (ananda balasana) stretches the inner groin (adductors) and hip rotators — muscles that directly connect to the pelvic floor via the fascial network. Releasing these surrounding tissues reduces the mechanical load on the pelvic floor itself.
- Lie on your back. On an exhale, draw both knees toward your chest.
- Open your knees wider than your torso and flex your feet toward the ceiling.
- Reach up and hold the outer edges of your feet (or use a yoga strap around each foot if reaching is difficult).
- Gently pull your feet downward while keeping your lower back pressed into the mat.
- Hold for 5–10 breath cycles, focusing on releasing the groin and pelvic floor with each inhale.
- You may gently rock side to side for an additional massaging effect.
Exercise 5: Supported Bridge with Pelvic Drop
Why it works: This is not a glute bridge — it is the opposite. Where a glute bridge aims to activate the gluteal muscles and compress the pelvic floor, this variation uses a yoga block or bolster under the sacrum to passively open and decompress the pelvic floor in a semi-inverted position.
- Lie on your back with knees bent. Lift your hips just enough to slide a yoga block (on its lowest height) or a folded blanket under your sacrum — the flat triangular bone at the base of your spine.
- Allow your hips to relax fully onto the support. Your pelvis should feel slightly tilted toward neutral.
- Completely release any tension in your glutes, inner thighs, and pelvic floor.
- Take 8–10 slow diaphragmatic breaths, imagining the pelvic floor opening with each inhale.
- Hold for 2–3 minutes. Remove the block slowly and rest in neutral for 30 seconds before moving.
Exercise 6: Progressive Muscle Relaxation of the Pelvic Floor
Why it works: Progressive muscle relaxation (PMR) is a well-established technique for releasing chronic muscle tension. By intentionally contracting a muscle group briefly and then fully releasing it, you train the nervous system to recognize and access the "off" state. For hypertonic pelvic floors, this contrast technique can break the cycle of chronic contraction [1].
- Lie comfortably on your back with knees bent.
- Take two slow breaths to settle.
- On an exhale, gently contract your pelvic floor muscles at about 30–40% of your maximum effort — just a mild squeeze. Hold for 3 seconds.
- Then fully release and let the muscles go completely limp. Breathe in slowly and feel the release deepen with the inhale. Rest for 10 seconds.
- Repeat 5 times. The goal is to make the contrast between "on" and "off" as clear as possible — the release phase is the therapeutic part.
Caution: If contracting even at low intensity triggers pain, skip this exercise and focus on breathing and yoga poses until some baseline relaxation has been achieved.
Exercise 7: Supine Butterfly with Diaphragm Breath
Why it works: The butterfly (baddha konasana) position gently stretches the adductors and the medial pelvic floor muscles. In the supine (lying down) version, gravity assists the release, making it accessible even for people in significant pain.
- Lie on your back. Bring the soles of your feet together and allow your knees to fall open to the sides in a diamond shape.
- Place a pillow or folded blanket under each knee if the stretch is too intense — the inner thighs should feel a gentle pull, not strain.
- Allow your arms to rest alongside your body, palms facing up.
- Take 10 slow diaphragmatic breaths. With each inhale, feel the pelvic floor soften and widen between the sit bones.
- Hold for 2–3 minutes. This exercise is particularly effective just before bed to release tension accumulated during the day.
4-Week Relaxation Protocol
Rushing into all seven exercises at once is counterproductive — the nervous system needs gradual retraining. Use this progressive protocol to build the foundation before adding complexity.
| Week | Focus | Exercises | Daily Time |
|---|---|---|---|
| Week 1 | Breathing foundation | Exercise 1 (diaphragmatic breathing) only — 4× daily | 10 min |
| Week 2 | Add active release | Exercise 1 + Exercise 2 (reverse kegel) + Exercise 6 (PMR) | 15–20 min |
| Week 3 | Add yoga-based stretches | Exercises 1, 2, 3 (child's pose), 4 (happy baby), 7 (butterfly) | 20–25 min |
| Week 4 | Full sequence | All 7 exercises in sequence — morning and evening sessions | 25–30 min |
Track your relaxation sessions with the free PelvicFit app — customizable hold and release timers, no account needed.
When Do Kegels Make It Worse?
Kegel exercises are the most widely recommended intervention for pelvic floor problems, and they are genuinely helpful — but only for a hypotonic (weak) pelvic floor. For a hypertonic floor, standard kegels are contraindicated in most cases, and performing them can significantly worsen symptoms.
Here is why: a kegel exercise is a maximal voluntary contraction of the pelvic floor. If the muscles are already in a state of chronic over-contraction, adding more contraction increases muscle tone further, reduces blood flow to the already-ischemic tissue, and amplifies pain signals. Many people with undiagnosed hypertonicity diligently perform kegels for months — because they read that kegels are good for the pelvic floor — only to find their pain, urgency, or discomfort steadily worsens. This is the kegel paradox.
The solution is to switch from kegel contractions to reverse kegel exercises and the relaxation protocol above. Most pelvic floor physical therapists will delay or eliminate kegel training entirely until the floor demonstrates the ability to fully relax at the end of a contraction. Only then — once the muscles can go from fully contracted to fully relaxed — is strengthening training introduced.
Signs that kegels are making your symptoms worse:
- Increased pelvic pain or pressure during or after exercises
- Worsening urinary urgency or frequency
- More pain during sex following a kegel session
- Muscle spasms or cramping in the pelvic region
- General increase in tension or discomfort in the days after practicing
If you experience any of these, stop kegels immediately and transition to the relaxation program above. Then see a pelvic floor physiotherapist for formal assessment. For a comprehensive comparison of kegels and reverse kegels, visit our pelvic floor FAQ.
When to See a Pelvic Floor Physical Therapist
The at-home relaxation program above is a strong starting point, but there are clear situations where professional support is essential. Seek a pelvic floor physiotherapist if:
- Your symptoms are severe or significantly limiting daily activities, work, or relationships
- You have tried relaxation exercises consistently for 4–6 weeks with no meaningful improvement
- Pain is worsening despite rest and relaxation practice
- You have a co-existing diagnosis of endometriosis, interstitial cystitis, or another pelvic condition
- You have a history of pelvic trauma, sexual trauma, or pelvic surgery
- You are experiencing vaginismus that prevents pelvic examinations or gynecological care
- You have developed anxiety or depression related to your pelvic pain
- You need confirmation of your diagnosis before committing to a treatment approach
A pelvic floor PT will perform an internal assessment to confirm tone, identify trigger points, provide manual therapy (including myofascial release and trigger point release), and create a personalized program. Many people with moderate-to-severe hypertonicity benefit from a combination of manual therapy and the home exercises described above — the two approaches complement each other effectively.
Frequently Asked Questions
How do you fix a hypertonic pelvic floor?
A hypertonic pelvic floor is treated with relaxation-focused techniques rather than strengthening. The first-line approach is diaphragmatic breathing combined with reverse kegel exercises — these retrain the nervous system to release the muscles. Yoga-based stretches (child's pose, happy baby, supine butterfly) add structural lengthening of the surrounding tissues. For moderate-to-severe cases, manual therapy from a pelvic floor physical therapist — including internal myofascial release and trigger point work — accelerates recovery significantly. Standard kegel contractions should be avoided until the muscles can fully relax.
How long does it take to heal a hypertonic pelvic floor?
Most people notice meaningful improvement within 6–12 weeks of consistent daily relaxation practice, particularly when combined with pelvic floor physiotherapy. Full resolution can take 3–6 months, depending on the severity of the tension, the underlying cause (trauma-related hypertonicity tends to take longer than posture-related cases), and whether co-existing conditions such as endometriosis are present. Consistency with diaphragmatic breathing — ideally 4 sessions daily — is the single biggest predictor of recovery speed. Some people see dramatic improvement within 2–3 weeks; others require longer. Progress is often non-linear, with flare-ups during stressful periods. Track your symptoms week by week rather than day by day.
Can kegel exercises make a hypertonic pelvic floor worse?
Yes, definitively. Kegel exercises add contraction force to muscles that are already in a state of chronic over-contraction. The result is increased muscle tone, reduced blood flow to ischemic tissue, amplified pain signals, and worsening of all associated symptoms — including pelvic pain, urinary urgency, and pain with sex. If you notice your symptoms worsening after performing kegels, this is one of the strongest clinical indicators of a hypertonic floor. Stop kegels, switch to reverse kegels and diaphragmatic breathing, and consult a pelvic floor physiotherapist for formal assessment.
What causes a hypertonic pelvic floor?
The most common causes are chronic psychological stress (which drives reflexive pelvic floor guarding, just as it drives jaw clenching), history of pelvic or sexual trauma, chronic pelvic pain conditions such as endometriosis or interstitial cystitis, high-impact sport with repetitive pelvic loading, habitual postural patterns including prolonged sitting and anterior pelvic tilt, and pelvic surgery or childbirth injury. In most cases, multiple factors are present simultaneously, which is why a comprehensive assessment — rather than treating one cause in isolation — produces the best outcomes.
References
- Faubion SS, Shuster LT, Bharucha AE. Recognition and management of nonrelaxing pelvic floor dysfunction. Mayo Clin Proc. 2012;87(2):187-193. doi:10.1016/j.mayocp.2011.09.004
- Cleveland Clinic. Pelvic Floor Dysfunction: Symptoms, Causes, Diagnosis & Treatment. Cleveland Clinic Health Library. Reviewed 2023. Available at: https://my.clevelandclinic.org/health/diseases/14459-pelvic-floor-dysfunction
- Torosis MD, Cohen D, Bhattacharya I, et al. Assessing the efficacy of pelvic floor muscle training in patients with pelvic floor hypertonicity: A systematic review. Female Pelvic Med Reconstr Surg. 2022;28(3):156-163. doi:10.1097/SPV.0000000000001114
Key Takeaways
- •A hypertonic pelvic floor is over-contracted, not weak — it requires relaxation, not strengthening exercises.
- •The 12 key symptoms include pelvic pain, painful sex, urinary urgency, constipation, tailbone pain, and worsening with kegels.
- •Standard kegel exercises are contraindicated for hypertonic floors and can significantly worsen all symptoms.
- •Diaphragmatic breathing is the most important first step — practice it 4 times daily to begin retraining pelvic floor relaxation.
- •Most people see meaningful improvement within 6–12 weeks of the relaxation protocol; a pelvic floor PT accelerates recovery in moderate-to-severe cases.
Track your pelvic floor relaxation progress
The PelvicFit app includes customizable hold and release timers for reverse kegel practice and relaxation sessions — free, no signup required.
Start your relaxation session →About the Authors
PelvicFit Editorial Team
The PelvicFit editorial team produces evidence-based content on pelvic floor health, drawing on peer-reviewed research and clinical guidelines from leading pelvic health organizations.
Sarah Mitchell, DPT — Pelvic Floor Physical Therapist (Reviewer)
Sarah holds a Doctor of Physical Therapy degree and has 12 years of clinical experience treating pelvic floor disorders, including hypertonic pelvic floor dysfunction, chronic pelvic pain, and vaginismus. She has treated over 800 patients across a range of pelvic floor conditions.