Pelvic Organ Prolapse: Stages 1–4, Symptoms & What You Can Do About It
Based on ACOG Practice Bulletin 214, Cochrane systematic reviews, and peer-reviewed urogynecology research. See our editorial standards.
Quick Answer
Pelvic organ prolapse (POP) occurs when the pelvic floor muscles and ligaments weaken, allowing pelvic organs to descend into the vaginal canal. It affects up to 50% of women who have given birth. Stages 1–2 are often managed without surgery. The key symptom is a feeling of heaviness or pressure in the vagina.
What Is Pelvic Organ Prolapse?
Pelvic organ prolapse occurs when the muscles, ligaments, and connective tissue that form the pelvic floor can no longer adequately support the organs they cradle — the bladder, uterus, rectum, and small intestine. When this supportive hammock weakens or tears, one or more of these organs can descend from their normal anatomical position into or beyond the vaginal canal.
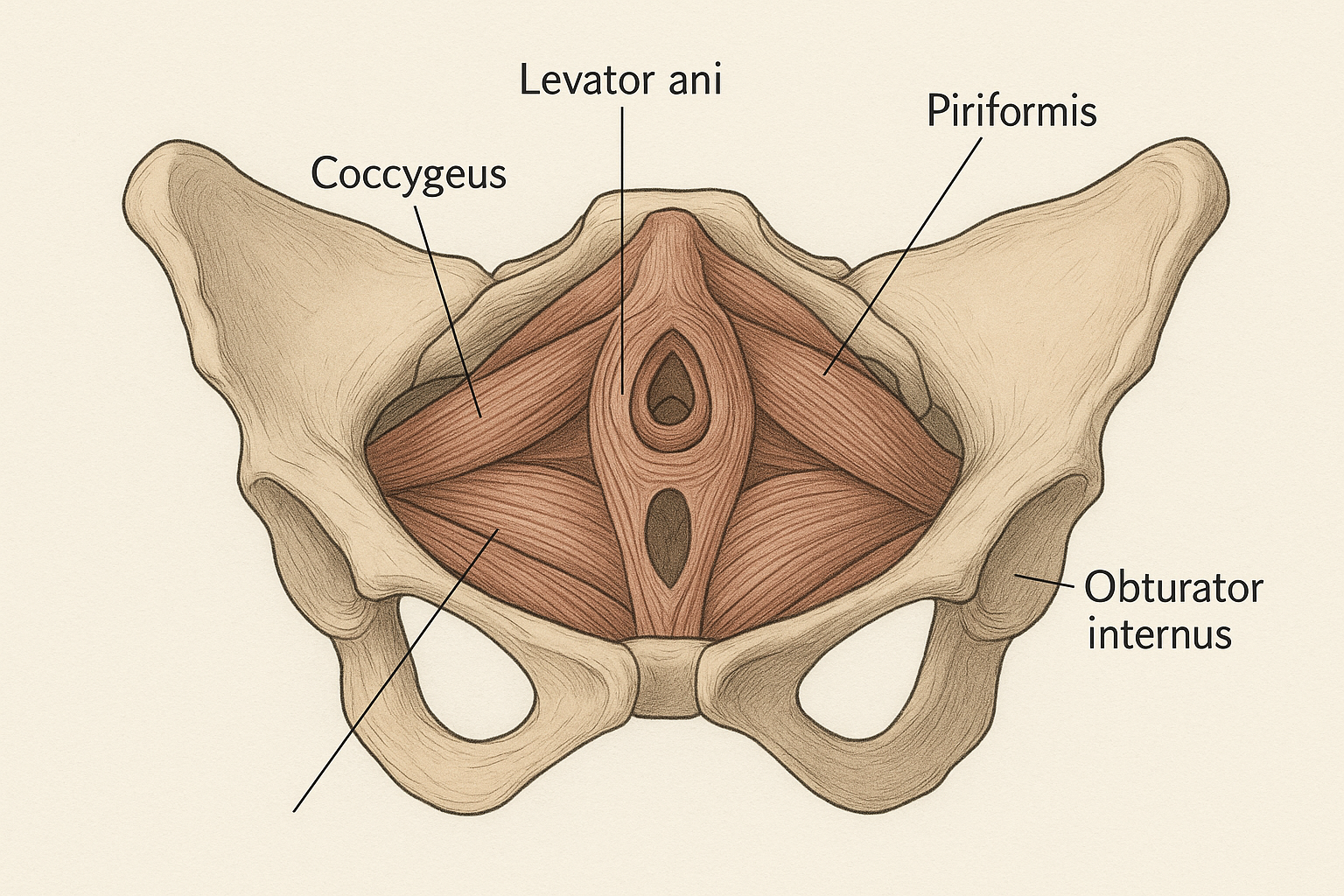
The pelvic floor is a remarkably complex structure. It is not a single muscle but a layered group of muscles (the levator ani complex and coccygeus), fascia, and ligaments that span the base of the pelvis from the pubic bone in front to the coccyx (tailbone) at the back. These structures must simultaneously support organs weighing several kilograms, coordinate with the abdominal muscles during exertion, and allow for the controlled opening and closing of the urethra and rectum. When any part of this system fails — due to childbirth injury, hormonal changes, chronic pressure, or genetic predisposition — prolapse can result.
The epidemiology of prolapse is striking. A landmark study by Olsen et al. found that women have an approximately 11% lifetime risk of undergoing surgery for prolapse or urinary incontinence [1]. More broadly, when clinical examination is used rather than self-report, up to 50% of parous women (women who have given birth) show some degree of prolapse — though many have no symptoms whatsoever. The condition is far more common than most women realize, which means you are not alone, and it is not a sign that something has gone catastrophically wrong with your body.
Prolapse is most common in women, but men can develop rectal prolapse (descent of the rectum). This article focuses primarily on female pelvic organ prolapse, which is the most prevalent and most studied form.
The 4 Types of Pelvic Organ Prolapse
Prolapse is categorized by which organ has descended and which wall of the vagina is affected. Understanding the type of prolapse you have matters because it influences both symptoms and the specific treatment approach recommended.
1. Cystocele (Bladder Prolapse) — The Most Common Type
A cystocele occurs when the bladder descends into and pushes against the anterior (front) vaginal wall, causing it to bulge downward. Because the bladder and the anterior vaginal wall are anatomically adjacent, any weakening of the pubocervical fascia — the connective tissue that holds the bladder in place — allows the bladder to sag. Cystocele is the most common type of prolapse and is frequently associated with symptoms of urinary urgency, frequency, incomplete bladder emptying, and recurrent urinary tract infections. Women sometimes describe a sensation as though they are sitting on a ball. Learn more in our guide on cystocele treatment without surgery.
2. Rectocele (Rectal Prolapse into the Vagina)
A rectocele occurs when the rectum bulges forward against the posterior (back) vaginal wall. It develops when the rectovaginal fascia — the connective tissue separating the rectum from the vagina — is weakened, typically through the forces of vaginal delivery. Rectocele is strongly associated with difficulty defecating: stool can become trapped in the bulge, leading many women to use a technique called "splinting" (pressing fingers against the vaginal wall or perineum) to assist evacuation. Bowel symptoms often feel embarrassing to discuss, but they are a recognized medical consequence of posterior wall prolapse, not a personal failing.
3. Uterine Prolapse
Uterine prolapse occurs when the uterus descends through the cervix toward or beyond the vaginal opening. The uterus is normally held in place by the cardinal and uterosacral ligaments, which can be overstretched during childbirth — particularly long labors, large babies, or instrumental deliveries. Mild uterine prolapse may cause a sensation of pelvic pressure or low back ache; severe prolapse can result in the uterus protruding completely outside the body (complete procidentia), a Stage 4 condition.
4. Vaginal Vault Prolapse
Vaginal vault prolapse is unique in that it occurs only in women who have had a hysterectomy (removal of the uterus). Once the uterus is removed, the top of the vagina (the "vault") must be surgically attached to supporting structures. If these attachments weaken or fail, the vaginal vault can descend — sometimes accompanied by portions of the bladder, rectum, or small intestine (enterocele). Vault prolapse affects approximately 1–2% of women after hysterectomy and may develop years after the original surgery.
The 4 Stages Explained Plainly
Clinicians use the POP-Q system — the Pelvic Organ Prolapse Quantification system, developed by the International Continence Society — to objectively measure and stage prolapse. The staging is based on the position of the leading edge of the prolapse relative to the hymenal ring (the remnants of the hymen, used as a fixed anatomical landmark). Here is what each stage means in plain language:
| Stage | Definition | Typical Symptoms | Treatment Options |
|---|---|---|---|
| Stage 1 | Leading edge is more than 1 cm above the hymen | Usually none; often found on routine exam | Lifestyle modification, pelvic floor exercises, monitoring |
| Stage 2 | Leading edge is within 1 cm above or below the hymen | Mild pelvic pressure, bladder/bowel changes, end-of-day heaviness | Pelvic floor training, pessary, lifestyle changes |
| Stage 3 | Leading edge extends more than 1 cm beyond the hymen | Visible bulge, significant urinary/bowel symptoms, discomfort with activity | Pessary, targeted PT; surgery often considered |
| Stage 4 | Complete or near-complete eversion of the vaginal wall | Severe symptoms, potential urinary retention, significant impact on daily life | Surgery typically required; pessary as bridge or for non-surgical candidates |
Staging based on the ICS POP-Q system. Stage does not always correlate with symptom severity — some Stage 2 women are more symptomatic than Stage 3.
An important nuance: staging does not always directly predict symptom severity. Some women with Stage 2 prolapse find symptoms highly distressing, while others with Stage 3 are relatively comfortable. Clinical decision-making is therefore guided by symptoms and their impact on quality of life, not stage alone. ACOG Practice Bulletin 214 explicitly states that asymptomatic prolapse does not require treatment.
Symptoms of Pelvic Organ Prolapse
The symptom picture of prolapse varies significantly depending on the type, stage, and which organs are involved. Below are the most common symptoms, along with an explanation of why each occurs:
1. Vaginal Heaviness or Pressure
The hallmark symptom. Women describe a dragging, bearing-down sensation in the pelvis or lower abdomen, often compared to the feeling of a period pain that never resolves. It results directly from the weight of the descended organ pulling on the vaginal walls and pelvic floor.
2. A Visible or Palpable Bulge at the Vaginal Opening
In Stage 3 and 4 prolapse, women may see or feel a bulge protruding from the vagina — particularly when straining or standing. Some notice it while bathing or when wiping after using the toilet. This is the prolapsed organ pressing through the vaginal opening.
3. Difficulty Emptying the Bladder
Particularly common with cystocele. The distorted anatomy can kink the urethra, meaning that the bladder never fully empties. Women may need to change position (leaning forward or pressing on the vaginal wall) to void completely. Incomplete emptying also increases the risk of urinary tract infections.
4. Urinary Urgency and Frequency
The prolapsed bladder may irritate the detrusor muscle (the bladder wall), triggering urgency — a sudden, compelling urge to urinate — and frequency, needing to void more than 8 times per day. This pattern overlaps with overactive bladder syndrome and can be misattributed if prolapse is not assessed.
5. Difficulty Defecating
With rectocele, stool can collect in the rectal bulge rather than moving forward toward the anus. This causes a sense of incomplete evacuation, excessive straining, and sometimes the complete inability to defecate without manual assistance.
6. Splinting to Evacuate the Bowel
As described above, many women with rectocele learn to press their fingers against the vaginal wall or perineum to "splint" the bulge and allow stool to pass normally. While effective, this behavior is a significant quality-of-life indicator and should be discussed with a healthcare provider.
7. Lower Back Pressure
The altered position of the pelvic organs places additional tension on the sacral and uterosacral ligaments, which can radiate as a low, dull ache in the lower back or sacrum. This symptom is often worse at the end of the day, when gravity has had maximal effect, and relieves with lying down.
8. Discomfort or Pain During Sex
Depending on the type and stage of prolapse, sexual intercourse may cause discomfort for the woman, and some partners can feel the prolapsed tissue. This can significantly affect sexual confidence and intimacy. Stage 1 and 2 prolapse rarely causes significant sexual dysfunction, while Stage 3 and 4 are more likely to interfere with comfortable intercourse.
9. Worsening Symptoms After Prolonged Standing or at Day's End
Gravitational loading accumulates throughout the day. Women with prolapse frequently report that symptoms are minimal or absent in the morning and worsen progressively through the afternoon and evening — or after activities like prolonged standing, walking, or exercise. Lying down provides relief because gravity no longer acts on the prolapsed tissue.
Important
Not all prolapse causes symptoms. Stage 1 is frequently discovered during routine pelvic examination with no symptoms at all. Treating an asymptomatic prolapse is generally not recommended — the goal is to prevent progression and preserve quality of life, not to treat an anatomical finding that is not causing distress.
Causes and Risk Factors
Prolapse is almost always multifactorial — no single cause is responsible in isolation. Understanding risk factors helps women make informed decisions about prevention, timing of interventions, and long-term management.
| Risk Factor | Relative Risk / Impact | Notes |
|---|---|---|
| Vaginal childbirth | Approximately ×4 increased risk | First vaginal delivery causes most pelvic floor injury; risk increases with each subsequent birth |
| Forceps or vacuum delivery | Approximately ×7 increased risk | Instrumental delivery significantly increases risk of levator ani avulsion (muscle tear) |
| BMI >30 | Approximately ×2 increased risk | Excess abdominal weight increases chronic downward pressure on pelvic floor |
| Family history (first-degree relative) | ~2.5× increased risk | Genetic factors influence connective tissue quality (collagen type III ratio) |
| Menopause (estrogen deficiency) | Significant contributor after age 50 | Estrogen maintains collagen and tissue elasticity; its loss accelerates tissue atrophy |
| Chronic straining (constipation, cough) | Cumulative risk over time | Repeated Valsalva maneuvers (straining) create sustained downward pressure on pelvic structures |
| Previous hysterectomy | 5× risk of vault prolapse specifically | Disrupts ligamentous support; risk varies with surgical technique |
It is worth emphasizing what is not on this list: normal-intensity exercise (including most forms of running and resistance training) does not cause prolapse in women with a functioning pelvic floor. The concern is specifically about high-impact activity undertaken on a pelvic floor that is already weakened or incompletely recovered — such as immediately after childbirth or after diagnosed prolapse without appropriate rehabilitation.
Can Pelvic Organ Prolapse Be Reversed?
This is the question most women ask first, and it deserves a precise, honest answer rather than a blanket reassurance or a scare.
Anatomical reversal — meaning the prolapsed organ returns fully to its pre-prolapse anatomical position — is generally not achievable without surgery for most women beyond Stage 1. The reason is structural: the connective tissue supports (fascia and ligaments) that have been stretched or torn do not regenerate fully through exercise alone, even when the muscles surrounding them strengthen significantly.
Symptom reversal, however, is a different story — and this is the clinically meaningful goal for most women. A 2011 Cochrane review by Hagen and Stark found that supervised pelvic floor muscle training significantly reduced prolapse symptoms and severity scores in women with Stage 1–2 prolapse [2]. Many women with Stage 1 or Stage 2 prolapse who complete a dedicated program report becoming entirely symptom-free. The prolapse may still be detectable on examination, but it no longer interferes with their daily life, exercise, or sexual function.
For Stage 3 and Stage 4 prolapse, conservative management can reduce symptoms and improve quality of life, but is rarely sufficient as a standalone treatment. Surgical options are typically discussed at these stages, particularly when urinary retention, significant bowel dysfunction, or severe quality of life impairment is present.
The bottom line: the goal of prolapse management is symptom-free living, not necessarily a normal anatomical exam. This is an achievable goal for the majority of women with Stage 1–2 prolapse through conservative means.
Conservative Treatment Options
ACOG Practice Bulletin 214 recommends that conservative (non-surgical) management be attempted before surgical referral is considered, except in cases of severe Stage 3–4 prolapse with significant functional impairment. Conservative options fall into four categories:
1. Pelvic Floor Muscle Training
Pelvic floor muscle training (PFMT) — sometimes called kegel exercises — is the cornerstone of conservative prolapse management. The 2011 Cochrane review by Hagen and Stark, which included 447 women across three trials, found that women who received supervised PFMT were significantly more likely to report improvement in prolapse symptoms and demonstrate reduced prolapse severity on examination compared to controls [2]. The key word in that evidence base is "supervised" — technique matters enormously. A study by Bump et al. found that 30% of women perform kegel exercises incorrectly even after verbal instruction. For technique guidance, see our complete guide on how to do kegel exercises.
2. Pessary Fitting
A pessary is a removable silicone device inserted into the vagina to mechanically support the prolapsed organs. Modern pessaries come in dozens of shapes and sizes and can be fitted by a gynecologist or urogynecologist. Many women use a pessary successfully for years — some preferring it permanently over surgery. Pessaries are particularly effective for women who want to remain active (running, exercising) without prolapse symptoms, and for those who are not surgical candidates due to age or health conditions. They require periodic removal and cleaning, typically every 3–6 months in a clinical setting.
3. Lifestyle Modification
Several lifestyle factors significantly affect prolapse severity and progression:
- Weight management: Even a 5–10% reduction in body weight reduces chronic pelvic floor loading. For women with BMI >30, this is one of the highest-impact interventions available.
- Treating constipation: Chronic straining at stool is one of the most damaging ongoing stressors for the pelvic floor. Increasing dietary fiber, hydration, and using stool softeners or osmotic laxatives when needed can dramatically reduce symptoms.
- Lifting technique: Learning to exhale and pre-contract the pelvic floor before and during any lift (the "brace and breathe" technique) prevents the spike in intra-abdominal pressure that drives prolapse downward during heavy exertion.
- Activity modification: High-impact exercise (running, jumping) should be temporarily modified or replaced with lower-impact alternatives (swimming, cycling) during the initial rehabilitation phase, then gradually reintroduced as pelvic floor strength improves.
4. Local Estrogen Therapy
For postmenopausal women, low-dose vaginal estrogen cream or suppositories can improve tissue quality around the vagina and pelvic floor — making both pessary fitting more comfortable and PFMT more effective. Discuss this option with your gynecologist; vaginal estrogen has an excellent safety profile and is not the same as systemic hormone therapy.
The Pelvic Floor Training Protocol for Prolapse
The following protocol is based on the Hagen Cochrane evidence and modified for prolapse — with an emphasis on the position progression (lying to standing) which is especially important for prolapse because gravity affects symptoms. Use the PelvicFit timer to track sets automatically.
| Parameter | Beginner (Weeks 1–4) | Intermediate (Weeks 5–12) | Maintenance (Week 13+) |
|---|---|---|---|
| Hold duration | 3–5 seconds | 5–8 seconds | 8–10 seconds |
| Rest between reps | Equal to hold (3–5 sec) | Equal to hold | 5–10 seconds |
| Reps per set | 8–10 | 10–15 | 10–15 |
| Sets per day | 2–3 | 3 | 3–4 days/week |
| Position | Lying down (gravity off) | Seated, then standing | Standing, functional positions |
| Quick contractions | Optional (5–8 reps) | Add 8–10 after slow holds | 10 after slow holds |
Protocol based on Hagen & Stark (2011) Cochrane review evidence and ACOG Practice Bulletin 214 recommendations. For postpartum recovery protocol, see our postpartum pelvic recovery guide.
Prolapse-specific tip
Always begin pelvic floor exercises lying down when managing prolapse. Gravity increases downward pressure on the pelvic organs in upright positions. As strength improves, progress to seated and then standing exercises — this position progression ensures you build enough strength to support the organs against gravity, which is the functional goal.
When Surgery Is Recommended
Surgery is not the first step for most women with prolapse, but it is the right step for some. ACOG guidelines and urogynecological consensus identify the following as criteria for surgical referral:
- Stage 3 or Stage 4 prolapse causing significant symptoms
- Conservative management (PFMT + pessary) tried for 3–6 months without adequate symptom relief
- Urinary retention (inability to fully empty the bladder) — this requires more urgent attention
- Quality of life severely affected despite optimal conservative management
- Patient preference after being fully informed of both surgical and non-surgical options
Common surgical approaches include:
- Colporrhaphy (anterior or posterior repair): Surgical reinforcement of the anterior or posterior vaginal wall. This is the most common repair for cystocele and rectocele. It uses the patient's own tissue and has good long-term outcomes in appropriate candidates.
- Sacrocolpopexy: Attachment of the vaginal vault to the sacrum using a synthetic or biological mesh bridge. Considered the gold standard for vault prolapse, with excellent long-term durability. This is most commonly performed laparoscopically or robotically.
- Sacrospinous ligament fixation: A vaginal approach to suspending the vaginal vault to the sacrospinous ligament. Less invasive than sacrocolpopexy but with somewhat higher recurrence rates.
A note on mesh: transvaginal mesh kits for prolapse repair were recalled by the FDA in 2019 due to serious complications. Abdominal mesh (used in sacrocolpopexy) has a different and substantially better safety profile and remains in common use. Discuss specific implant types with your surgeon if mesh is part of your proposed treatment plan.
Sex and Relationships With Prolapse
Sexual activity with prolapse is a topic many women feel reluctant to raise with their healthcare provider — but it is one of the most significant quality-of-life concerns associated with the condition, and it deserves direct discussion.
Most women with Stage 1–2 prolapse are able to have comfortable, fulfilling sexual intercourse. At these stages, the prolapsed tissue typically reduces (returns upward) in the lying-down position, which means it is often not present or detectable during sex. Some women notice no difference in sexual experience whatsoever after a Stage 1–2 diagnosis.
For women with more significant prolapse, certain positions tend to minimize discomfort:
- Lying on your back with a pillow under your hips allows gravity to reduce the prolapse and may make intercourse more comfortable.
- Side-lying positions reduce downward gravitational pressure and are often better tolerated than upright positions.
- Woman-on-top positioning gives you more control over depth and angle, which can reduce discomfort if certain positions feel uncomfortable.
Some partners may be able to feel the prolapsed tissue during sex. This is worth discussing openly rather than letting it become a source of anxiety or avoidance for either partner. A pelvic floor physiotherapist can provide specific guidance on sexual positioning and address concerns about pain (dyspareunia) that sometimes accompanies prolapse.
If penetrative sex is uncomfortable, a pessary can sometimes be used during intercourse — certain ring-type pessaries are designed for this purpose. This is worth discussing with the clinician who fitted your pessary.
Frequently Asked Questions
How do you know if you have pelvic organ prolapse?
The most common symptom is a sensation of heaviness, pressure, or bulging in the vagina — often described as "something falling out." Other signs include a visible or palpable bulge at or beyond the vaginal opening, difficulty emptying the bladder or bowel completely, lower back pressure that worsens at day's end or after prolonged standing, and pain or discomfort during sex. Many Stage 1 prolapses are entirely asymptomatic and discovered during a routine pelvic exam. If you suspect prolapse, a pelvic examination by your gynecologist or a pelvic floor physiotherapist can confirm the diagnosis and staging.
Can you heal pelvic organ prolapse naturally?
Stage 1 and Stage 2 prolapse can often be managed effectively — and symptoms fully controlled — without surgery using pelvic floor muscle training, pessary support, weight management, constipation treatment, and activity modification. Anatomical reversal (the organ returning to its original position) is usually not possible without surgery. However, the key goal is symptom-free living, which conservative treatment achieves for many women with mild-to-moderate prolapse. ACOG recommends conservative management first before surgical referral.
What makes pelvic organ prolapse worse?
The factors most likely to worsen prolapse are: chronic constipation and straining (which increases downward pressure significantly), heavy lifting without proper pelvic floor support, high-impact exercise before the pelvic floor is strong enough to handle it, excess body weight, chronic cough (from smoking or respiratory illness), and estrogen deficiency after menopause which reduces tissue elasticity. Managing these modifiable factors is as important as pelvic floor exercises in a comprehensive prolapse management plan.
Is pelvic organ prolapse dangerous?
Pelvic organ prolapse is not dangerous in the sense of being life-threatening in most cases. However, severe Stage 4 prolapse can interfere with bladder and bowel function, cause urinary retention (inability to void), and significantly impact quality of life. Any prolapse that causes inability to urinate is a medical emergency requiring prompt evaluation. Uterine prolapse rarely causes direct organ damage, but untreated complete procidentia (Stage 4 uterine prolapse) can lead to ulceration of the exposed vaginal tissue over time.
What are the 4 stages of pelvic organ prolapse?
Using the POP-Q staging system: Stage 1 — the leading edge of the prolapse is more than 1 cm above the hymen (often completely asymptomatic); Stage 2 — the leading edge is within 1 cm above or below the hymen (mild symptoms, well-managed conservatively); Stage 3 — the leading edge extends more than 1 cm below the hymen (visible bulge, significant symptoms, pessary or surgery often considered); Stage 4 — complete eversion of the vaginal wall (severe, almost always requires intervention). See the staging table above for a full breakdown.
References
- Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 1997;89(4):501-506.
- Hagen S, Stark D. Conservative prevention and management of pelvic organ prolapse in women. Cochrane Database Syst Rev. 2011;(12):CD003882.
- American College of Obstetricians and Gynecologists. Pelvic Organ Prolapse: ACOG Practice Bulletin, Number 214. Obstet Gynecol. 2019;134(5):e126-e142.
Key Takeaways
- 1. Pelvic organ prolapse affects up to 50% of women who have given birth, but most cases are Stage 1–2 and produce no or minimal symptoms.
- 2. There are 4 main types (cystocele, rectocele, uterine, vault) and 4 stages — staging is based on the POP-Q system and guides treatment planning.
- 3. Stage 1–2 prolapse is successfully managed without surgery in most women through pelvic floor training, pessary, and lifestyle changes.
- 4. Anatomical reversal without surgery is usually not achievable, but symptom-free living is the realistic and achievable clinical goal.
- 5. Managing chronic straining, excess weight, and high-impact activity is as important as pelvic floor exercises in slowing prolapse progression.
Start the PelvicFit Pelvic Floor Training Program
Designed by physiotherapists for prolapse management and prevention. Follow a structured program that progresses at the right pace — from lying to standing to functional exercises.
Start the free programAbout the Authors
PelvicFit Editorial Team
The PelvicFit editorial team produces evidence-based content on pelvic floor health, drawing on peer-reviewed research, clinical guidelines, and the expertise of our medical advisory board.
Sarah Mitchell, DPT — Reviewer, Physical Therapist specializing in pelvic floor dysfunction
Sarah holds a Doctor of Physical Therapy degree and has 12 years of clinical experience treating pelvic floor disorders including prolapse, incontinence, and postpartum recovery. She has treated over 800 patients and lectures on evidence-based pelvic floor rehabilitation.